You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.

AD1184
Celestial
Denis Staunton, writing in the Irish Times, has pegged that although Britain is one of the worst-affected countries in Europe, with a daily death toll that is still potentially accelerating, Boris Johnson has been able to rally the support of the British people behind his stupid slogan of 'Protect the NHS'. This widespread public approval is starkly at odds with the reality of terrible decisions, cowardly leadership and sluggishness that has been directly responsible for this terrible outcome, and which has placed the NHS under such strain:
NHS mythology shields Boris Johnson from coronavirus mistakes
There is now a weekly orgy of idiocy in this country where people are encouraged to bang pots and pans out of their window every Thursday night. Called 'Clap for Carers', this is to 'show support' for the NHS. A few weeks ago, the outgoing leader of the Labour Party, the elderly and officially vulnerable Jeremy Corbyn, was seen banging a drum on the street outside of his house. He was also filmed approaching other people for them to bang the drum. This festival has now reached such heights of idiocy that these were the embarrassing scenes on Westminster Bridge, just outside the Houses of Parliament this Thursday:
Coronavirus UK: Cressida Dick joins crowds clapping NHS | Daily Mail Online
These people are entirely clueless about what doing real favours for NHS workers would actually entail. For one, it would entail not mingling in large crowds and giving those workers a greater caseload to deal with in a few weeks' time. That the Met Police Commisioner Cressida Dick is among them for a photo op ought to lead to her sacking. She has been 'failing upwards' in the Met for too long.
NHS mythology shields Boris Johnson from coronavirus mistakes
There is now a weekly orgy of idiocy in this country where people are encouraged to bang pots and pans out of their window every Thursday night. Called 'Clap for Carers', this is to 'show support' for the NHS. A few weeks ago, the outgoing leader of the Labour Party, the elderly and officially vulnerable Jeremy Corbyn, was seen banging a drum on the street outside of his house. He was also filmed approaching other people for them to bang the drum. This festival has now reached such heights of idiocy that these were the embarrassing scenes on Westminster Bridge, just outside the Houses of Parliament this Thursday:
Coronavirus UK: Cressida Dick joins crowds clapping NHS | Daily Mail Online
These people are entirely clueless about what doing real favours for NHS workers would actually entail. For one, it would entail not mingling in large crowds and giving those workers a greater caseload to deal with in a few weeks' time. That the Met Police Commisioner Cressida Dick is among them for a photo op ought to lead to her sacking. She has been 'failing upwards' in the Met for too long.
Last edited:
AD1184
Celestial
That other coronaviruses circulating among the human population do not afford a lasting immunity was known before the Covid-19 pandemic reached these shores. That the government bet the farm on the assumption of immunity is one of many national scandals coming out of this epidemic. The paper that supposedly caused the government to change tack and institute a lockdown, from Imperial College epidemic modellers, is also based upon the same assumption.There is 'no evidence' that people who have survived coronavirus have immunity - WHO warns - after Britain 'paid £16m' for two million antibody tests from China that DON'T WORK
There is currently no evidence to support the belief that people who have recovered from coronavirus are immune to catching the virus again, the World Health Organisation has said. Senior WHO epidemiologists warned despite the hopes governments across the world have piled on antibody tests, there is no proof those who have been infected cannot be infected again.
The British Government has bought 3.5 million serology tests, which measure levels of antibodies in blood plasma, even though they are not definitive of growing levels of herd immunity. Many tests being developed are pin prick blood tests similar to widely used instant HIV tests and measure for raised levels of the antibodies the body uses to fight the virus.
Speaking at a press conference in Geneva, Dr Maria van Kerkhove said: 'There are a lot of countries that are suggesting using rapid diagnostic serological tests to be able to capture what they think will be a measure of immunity. 'Right now, we have no evidence that the use of a serological test can show that an individual has immunity or is protected from reinfection.' She added: 'These antibody tests will be able to measure that level of seroprevalence - that level of antibodies but that does not mean that somebody with antibodies means that they are immune.'
The Imperial College team used a compartmental model, or SIR model, of disease spread. The letters SIR are an abbreviation giving the 'compartments' that people are put into.
- S is the susceptible population.
- I is the infectious population (i.e. those who have the virus and are shedding, so can infect others).
- R is the removed population (those who have died of the disease, those who have been isolated and cannot infect others, or those who have had the disease, recovered and are now immune).
But if Covid-19 does not provide a lasting immunity, then the cycle through compartments might look like this: S → I → R → S → I → R → S ... Where the duration in the R compartment is of unknown length (possibly short). If there is no immunity at all, then the cycle is like this S → I → S → I → S ... until death. Existing coronaviruses are somewhat like this, where the immunity is only short-lived, or not even present, and they return seasonally.
This sort of modelling I have seen described as sophisticated in the press, by journalists who are evidently unfamiliar with mathematics. I would say that it is fairly crude, and the results you get out are tuned by an array of parameters whose values are informed by guesswork. They are useful educational tools for showing people what an epidemic trajectory looks like qualitatively, but I would not rest the fate of nations upon their results.
The very same academic unit whose model is said to have influenced the British government's policy (and the US government's) used similar modelling which lead British authorities to slaughter millions of healthy livestock in response to the 2001 foot and mouth epidemic. What is now widely viewed to have been a mistake which caused serious economic damage (at least, serious in pre-Covid-19 terms).
The whole thing goes to show that the government's mantra that its decisions have been guided 'by the science' is a nonsense. Science is not a monolithic entity. Science is a set of tools and a philosophy for discovering truths about the natural world. Science is also a collection of individuals across a vast array of disciplines, each with their own opinions about what those truths are. Scientists sometimes form consensuses on issues. Sometimes they divide into different schools of thought.
It is quite clear that what 'the science' says depends on whom you ask. There have been great differences between what government advisers have said, and what other equally qualified people have said. 'The science' on Covid-19 also differs from country to country (q.v. disparate national advice about the use of PPE by the general population, and differing views on the importance of community testing). It would be more truthful for the government to say that its decisions have been informed by the assumptions and judgements (even in the face of a lack of real scientific information about the threat) of a few scientists. These have often not fallen on the side of caution.
On another note, I do not agree with the quoted article's implication that the government should not begin widespread antibody testing until immunity is proven ("even though they are not definitive of growing levels of herd immunity"). For one thing, widespread antibody testing is useful for testing the hypothesis that there is an immunity to Covid-19 after infection. For another, it will show how far the infection has already spread in the country, which would be useful to a determination of the true infection fatality rate and reproduction number, and also for making better projections and plans.
Last edited:
Dejan Corovic
As above, so bellow
There are some good news:
Remdesivir: Covid-19 patients recovering quickly after getting experimental drug - CNN
"The patients taking part in a clinical trial of the drug have all had severe respiratory symptoms and fever, but were able to leave the hospital after less than a week of treatment, STAT quoted the doctor leading the trial as saying."
Remdesivir: Covid-19 patients recovering quickly after getting experimental drug - CNN
"The patients taking part in a clinical trial of the drug have all had severe respiratory symptoms and fever, but were able to leave the hospital after less than a week of treatment, STAT quoted the doctor leading the trial as saying."
nivek
As Above So Below
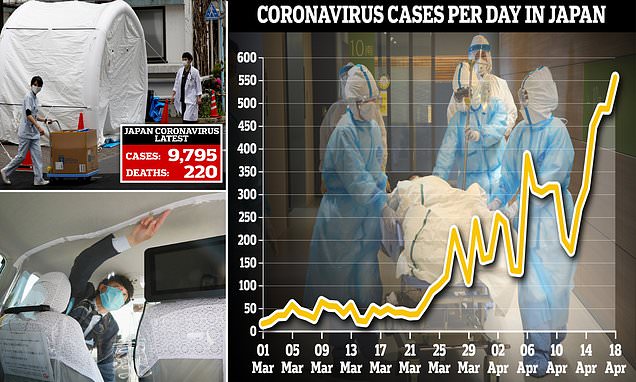
New wave of infections threatens to collapse Japan hospitals as they are forced to turn away sick people
In one recent case, an ambulance carrying a man with a fever and difficulty breathing was rejected by 80 hospitals (top left, medics walk by coronavirus testing tents at Kawakita General Hospital in Tokyo) and was forced to search for hours for a hospital in downtown Tokyo that would treat him. On Saturday, the number of cases rose from 9,239 yesterday to 9,795 and there have now been 220 deaths from the virus, up from 136 deaths on Friday. With an addition of 712 others from a cruise ship quarantined near Tokyo earlier this year, Japan now has 10,507 cases altogether (right, coronavirus cases per day in Japan). Nearly one-third of the domestic cases come from Tokyo, where the daily surge has overburdened hospitals. Another feverish man finally reached a hospital after paramedics unsuccessfully contacted 40 clinics. Pictured bottom left: A taxi driver displays a vinyl curtain installed between the driver's seat and the back seat as a preventative measure against coronavirus in Fukuoka on Saturday.
In one recent case, an ambulance carrying a man with a fever and difficulty breathing was rejected by 80 hospitals (top left, medics walk by coronavirus testing tents at Kawakita General Hospital in Tokyo) and was forced to search for hours for a hospital in downtown Tokyo that would treat him. On Saturday, the number of cases rose from 9,239 yesterday to 9,795 and there have now been 220 deaths from the virus, up from 136 deaths on Friday. With an addition of 712 others from a cruise ship quarantined near Tokyo earlier this year, Japan now has 10,507 cases altogether (right, coronavirus cases per day in Japan). Nearly one-third of the domestic cases come from Tokyo, where the daily surge has overburdened hospitals. Another feverish man finally reached a hospital after paramedics unsuccessfully contacted 40 clinics. Pictured bottom left: A taxi driver displays a vinyl curtain installed between the driver's seat and the back seat as a preventative measure against coronavirus in Fukuoka on Saturday.
nivek
As Above So Below
On another note, I do not agree with the quoted article's implication that the government should not begin widespread antibody testing until immunity is proven ("even though they are not definitive of growing levels of herd immunity"). For one thing, widespread antibody testing is useful for testing the hypothesis that there is an immunity to Covid-19 after infection. For another, it will show how far the infection has already spread in the country, which would be useful to a determination of the true infection fatality rate and reproduction number, and also for making better projections and plans.
Things keep pointing back to this, the need to test everyone and as promptly as we can across the world, we could know so much more about this virus as you mentioned and we need this information, especially we need to know if there is a true immunity to Covid-19 after infection, if there's not then our uphill battle against this virus will be obviously even more difficult...IMO
...
nivek
As Above So Below
No matter how you crunch the numbers, this pandemic is only just getting started
People are understandably looking for good news. But the truth is, we’re nowhere near controlling coronavirus.
(More on the link)
.
People are understandably looking for good news. But the truth is, we’re nowhere near controlling coronavirus.
(More on the link)
.
baleeber
Adept
That's an excellent assessment, and I agree with you. It seems to me that COVID-19 just keeps coming back, and that our original ideas of a vaccine may have been optimistic, to say the least.That other coronaviruses circulating among the human population do not afford a lasting immunity was known before the Covid-19 pandemic reached these shores. That the government bet the farm on the assumption of immunity is one of many national scandals coming out of this epidemic. The paper that supposedly caused the government to change tack and institute a lockdown, from Imperial College epidemic modellers, is also based upon the same assumption.
The Imperial College team used a compartmental model, or SIR model, of disease spread. The letters SIR are an abbreviation giving the 'compartments' that people are put into.
The assumption of these models is those who get infected move from the S compartment to the I compartment. When the disease runs its course in those, they move from the I compartment to the R compartment. Eventually S becomes zero, or so small that the reproduction number is insufficient to maintain transmission (the herd immunity we have all been told about), and the size of S holds steady, and all of the I is converted to R and the epidemic ends. That is, that the movement for an individual is S → I → R and then ends. Although populations are whole numbers of individuals, an assumption of these models is that when the numbers are very large, that you can model populations as continuous quantities. Also, S + I + R is a constant.
- S is the susceptible population.
- I is the infectious population (i.e. those who have the virus and are shedding, so can infect others).
- R is the removed population (those who have died of the disease, those who have been isolated and cannot infect others, or those who have had the disease, recovered and are now immune).
But if Covid-19 does not provide a lasting immunity, then the cycle through compartments might look like this: S → I → R → S → I → R → S ... Where the duration in the R compartment is of unknown length (possibly short). If there is no immunity at all, then the cycle is like this S → I → S → I → S ... until death. Existing coronaviruses are somewhat like this, where the immunity is only short-lived, or not even present, and they return seasonally.
This sort of modelling I have seen described as sophisticated in the press, by journalists who are evidently unfamiliar with mathematics. I would say that it is fairly crude, and the results you get out are tuned by an array of parameters whose values are informed by guesswork. They are useful educational tools for showing people what an epidemic trajectory looks like qualitatively, but I would not rest the fate of nations upon their results.
The very same academic unit whose model is said to have influenced the British government's policy (and the US government's) used similar modelling which lead British authorities to slaughter millions of healthy livestock in response to the 2001 foot and mouth epidemic. What is now widely viewed to have been a mistake which caused serious economic damage (at least, serious in pre-Covid-19 terms).
The whole thing goes to show that the government's mantra that its decisions have been guided 'by the science' is a nonsense. Science is not a monolithic entity. Science is a set of tools and a philosophy for discovering truths about the natural world. Science is also a collection of individuals across a vast array of disciplines, each with their own opinions about what those truths are. Scientists sometimes form consensuses on issues. Sometimes they divide into different schools of thought.
It is quite clear that what 'the science' says depends on whom you ask. There have been great differences between what government advisers have said, and what other equally qualified people have said. 'The science' on Covid-19 also differs from country to country (q.v. disparate national advice about the use of PPE by the general population, and differing views on the importance of community testing). It would be more truthful for the government to say that its decisions have been informed by the assumptions and judgements (even in the face of a lack of real scientific information about the threat) of a few scientists. These have often not fallen on the side of caution.
On another note, I do not agree with the quoted article's implication that the government should not begin widespread antibody testing until immunity is proven ("even though they are not definitive of growing levels of herd immunity"). For one thing, widespread antibody testing is useful for testing the hypothesis that there is an immunity to Covid-19 after infection. For another, it will show how far the infection has already spread in the country, which would be useful to a determination of the true infection fatality rate and reproduction number, and also for making better projections and plans.
baleeber
Adept
Yeah, that's what I think. Unfortunately, I agree with AD1184, who made a good point that Japan may not be seeing a second wave, but rather a delayed 1st wave, and I think we're about to get smacked down hard.No matter how you crunch the numbers, this pandemic is only just getting started
People are understandably looking for good news. But the truth is, we’re nowhere near controlling coronavirus.
(More on the link)
.
baleeber
Adept
But Nivek, if you test everyone, you're only going to find that almost everybody has it ...except, as you mention, a very small number of truly immune.Things keep pointing back to this, the need to test everyone and as promptly as we can across the world, we could know so much more about this virus as you mentioned and we need this information, especially we need to know if there is a true immunity to Covid-19 after infection, if there's not then our uphill battle against this virus will be obviously even more difficult...IMO
...
This was such an alarming statement that I spent a couple of hours today checking it out, and it's not true - virologists discovered that the SARS and MERS coronaviruses induce antibodies that are detectable in the patient's blood for about 24 and 18 months [1], and it's believed that these antibodies confer immunity during that time, but this assumption is untested. It is reasonable to tentatively conclude however that since the patients did recover from the virus, the antibodies played a role in their recovery.That other coronaviruses circulating among the human population do not afford a lasting immunity was known before the Covid-19 pandemic reached these shores. That the government bet the farm on the assumption of immunity is one of many national scandals coming out of this epidemic. The paper that supposedly caused the government to change tack and institute a lockdown, from Imperial College epidemic modellers, is also based upon the same assumption.
However early clinical results have indicated that the convalescent plasma harvested from recovered COVID-19 patients is effective in treating severely ill patients, and several studies are going on right now to quantify the benefits and any associated risks:
"COVID-19 is currently a big threat to global health. However, no specific antiviral agents are available for its treatment. In this work, we explore the feasibility of convalescent plasma (CP) transfusion to rescue severe patients. The results from 10 severe adult cases showed that one dose (200 mL) of CP was well tolerated and could significantly increase or maintain the neutralizing antibodies at a high level, leading to disappearance of viremia in 7 d. Meanwhile, clinical symptoms and paraclinical criteria rapidly improved within 3 d. Radiological examination showed varying degrees of absorption of lung lesions within 7 d. These results indicate that CP can serve as a promising rescue option for severe COVID-19, while the randomized trial is warranted."
Source: "Effectiveness of convalescent plasma therapy in severe COVID-19 patients," Kai Duan et al., PNAS, 4/6/2020
So it looks like we don't have any reason to freak out about unproven acquired immunity at this point, and we have good reason to hope that convalescent plasma treatments will save lives and confer a significant period of immunity to patients.
[1] "For patients with severe acute respiratory syndrome coronavirus (SARS-CoV) infection, antibodies persist for at least 2 years after symptomatic infection (2). Recently, antibodies against MERS-CoV were found (by ELISA and IFA) in 9 healthcare workers in Saudi Arabia with symptomatic MERS-CoV infection at least 18 months after infection (3). Duration of antibody responses beyond 18 months has not been reported (4)."
Source: "Persistence of antibodies against Middle East respiratory syndrome coronavirus," Payne et al., Emerg Infect Dis. 10/22/2016.
The results just came in from a random sampling of 3,000 residents of Santa Clara, California, and they found that only 2.5% - 4.2% of that population had been exposed to the virus (they tested positive for the antibodies to the SARS-CoV-2 virus) - that's far more than the official counts indicated, but nowhere near the entire population:But Nivek, if you test everyone, you're only going to find that almost everybody has it ...except, as you mention, a very small number of truly immune.
"Way more people may have gotten coronavirus than we are detecting.
That's the takeaway from a small study of coronavirus antibodies in more than 3,000 people in Santa Clara County, California. The results suggested that between 2.5% and 4.2% of people in the county have contracted COVID-19, which is 50 to 85 times greater than the number of cases being reported at the time. Not everyone is convinced the true prevalence is that high, however, with some saying the antibody test the researchers used was not reliable.
However, this type of antibody testing, or serologic study, should be rolled out more broadly, epidemiologists told Live Science."
Source: COVID-19 numbers in this California County may be way underestimated, small antibody study shows | Live Science
As far as we know, nobody is immune to this virus, but we have very good reasons to believe that recovered patients are immune for a period of time.
AD1184
Celestial
There is this study here from 1990:This was such an alarming statement that I spent a couple of hours today checking it out, and it's not true - virologists discovered that the SARS and MERS coronaviruses induce antibodies that are detectable in the patient's blood for about 24 and 18 months [1], and it's believed that these antibodies confer immunity during that time, but this assumption is untested. It is reasonable to tentatively conclude however that since the patients did recover from the virus, the antibodies played a role in their recovery.
However early clinical results have indicated that the convalescent plasma havrested from recovered COVID-19 patients is effective in treating severely ill patients, and several studies are going on right now to quantify the benefits and any associated risks:
The time course of the immune response to experimental coronavirus infection of man.
The time course of the immune response to experimental coronavirus infection of man.
K. A. Callow, H. F. Parry, M. Sergeant, and D. A. Tyrrell
Abstract
After preliminary trials, the detailed changes in the concentration of specific circulating and local antibodies were followed in 15 volunteers inoculated with coronavirus 229E. Ten of them, who had significantly lower concentrations of pre-existing antibody than the rest, became infected and eight of these developed colds. A limited investigation of circulating lymphocyte populations showed some lymphocytopenia in infected volunteers. In this group, antibody concentrations started to increase 1 week after inoculation and reached a maximum about 1 week later. Thereafter antibody titres slowly declined. Although concentrations were still slightly raised 1 year later, this did not always prevent reinfection when volunteers were then challenged with the homologous virus. However, the period of virus shedding was shorter than before and none developed a cold. All of the uninfected group were infected on re-challenge although they also appeared to show some resistance to disease and in the extent of infection. These results are discussed with reference to natural infections with coronavirus and with other infections, such as rhinovirus infections.
The researchers inoculated 15 volunteers with coronavirus 229E, ten became infected, eight developed colds. 14 of these were able to return a year later to be re-inoculated. The group of five originally uninfected became infected this time, and one developed a cold. Of 9 returning volunteers in the infected group, six became infected on inoculation and shed virus, but did not develop disease (i.e. they were potentially asymptomatic spreaders).
I think that the degree and duration of immunity conferred by antibodies will vary across the population because not everyone has the same immune response. Some diseases have a much better immune response that is more uniform across the population than others.
For the results in regards to SARS-Cov-2, there was this report on a medical pre-print from China that I posted a couple of weeks ago:
Low antibody levels raise questions about coronavirus reinfection risk
The pre-print is here:
Neutralizing antibody responses to SARS-CoV-2 in a COVID-19 recovered patient cohort and their implications
Researchers measured SARS-Cov-2-specific neutralizing antibody levels in recovered mild Covid-19 cases. They found that a third had levels that might be insufficient to prevent re-infection, and in some patients they could not detect antibodies. The researchers excluded severe cases because they could have been in receipt of antibody-containing blood plasma. The older patients tended to have a greater presence of neutralizing antibodies than younger ones.
The idea that those vulnerable to the severe illness will be able to rely upon the herd immunity offered by those less vulnerable therefore seems questionable to me. It also makes a vaccine's likelihood of succeeding similarly questionable. Some vaccines are able to prevent disease in an individual, but not infection, allowing them to keep spreading it. This was the cause of an argument between the WHO and China about 15 years ago, because the Chinese were vaccinating chickens against avian influenza, but their vaccines were only able to prevent disease in chickens, and not infection. This enabled asymptomatic spread and provided a breeding ground for avian flu to mutate into more dangerous strains.
We can only hope that there are other immune mechanisms at work that provide immunity to SARS-Cov-2 and that a vaccine will be successful, but assuming things is dangerous.
Last edited:
I'm very encouraged to see that small-scale study reporting successful outcomes with convalescent plasma: it sounds like they were able to pull several of those ten people back from the brink with just one injection. That's exactly what we need: a treatment that we can give to the most severe cases, and ideally reduce the chances of death in severe cases down to a few percent or less. Because that's what's really scaring the shit out of everyone: knowing that if this virus hits you hard and you get ARDS, then there's nothing they can do but put you on a ventilator and you'll have about a 20% chance of surviving. Yikes, y'know?There is this study here from 1990:
The time course of the immune response to experimental coronavirus infection of man.
The researchers inoculated 15 volunteers with coronavirus 229E, ten became infected, eight developed colds. 14 of these were able to return a year later to be re-inoculated. The group of five originally uninfected became infected this time, and one developed a cold. Of 9 returning volunteers in the infected group, six became infected on inoculation and shed virus, but did not develop disease (i.e. they were potentially asymptomatic spreaders).
I think that the degree and duration of immunity conferred by antibodies will vary across the population because not everyone has the same immune response. Some diseases have a much better immune response that is more uniform across the population than others.
For the results in regards to SARS-Cov-2, there was this report on a medical pre-print from China that I posted a couple of weeks ago:
Low antibody levels raise questions about coronavirus reinfection risk
The pre-print is here:
Neutralizing antibody responses to SARS-CoV-2 in a COVID-19 recovered patient cohort and their implications
Researchers measured SARS-Cov-2-specific neutralizing antibody levels in recovered mild Covid-19 cases. They found that a third had levels that might be insufficient to prevent re-infection, and in some patients they could not detect antibodies. The researchers excluded severe cases because they could have been in receipt of antibody-containing blood plasma. The older patients tended to have a greater presence of neutralizing antibodies than younger ones.
The idea that those vulnerable to the severe illness will be able to rely upon the herd immunity offered by those less vulnerable therefore seems questionable to me. It also makes a vaccine's likelihood of succeeding similarly questionable. Some vaccines are able to prevent disease in an individual, but not infection, allowing them to keep spreading it. This was the cause of an argument between the WHO and China about 15 years ago, because the Chinese were vaccinating chickens against avian influenza, but their vaccines were only able to prevent disease in chickens, and not infection. This enabled asymptomatic spread and provided a breeding ground for avian flu to mutate into more dangerous strains.
We can only hope that there are other immune mechanisms at work that provide immunity to SARS-Cov-2 and that a vaccine will be successful, but assuming things is dangerous.
The low antibody count in that third of recovered patients is odd and inconvenient, but it's not a big blow to the convalescent plasma approach - they can run an antibody titer on each donor and weed out the low-antibody producers, or just harvest what they can and increase the concentration of antibodies later.
I think the antibody approach is the most promising glimmer of hope that I've seen since all of this started. Within two weeks we'll know the stats on convalescent plasma treatments for severe cases, and at the end of May we'll have the results on its efficacy in moderate cases. And then there are the five synthetic antibodies by Distributed Bio that exhibited aggressive binding to the spike glycoprotein - if that works safely in vivo then it could be a game changer because those can be produced quickly and in large volumes, and save the lives of people teetering on the edge. A vaccine can't do that; it takes too much time to work. The gossip about remdesivir is sounding encouraging too, but it seems pretty experimental so I'm trying not to get my hopes up too high on that one.
I'll leave it with that thought, so I can get a decent sleep for a change: in a few weeks we could be hearing lots of stories about people being saved from a torturous death by a single injection of convalescent plasma. Frankly I've been going out of my mind for the last month looking for some ray of rational hope that we might be able to start helping the hundreds of thousands of unfortunate people who take a bad turn with this virus. So far this comes closer than anything: I'll take it. Because the trajectory of this pandemic at the global scale is the most chilling thing I've ever seen, and it helps to have some tangible sprig of hope to cling to when you look at this:

AD1184
Celestial
I don't think this is true. Why do you think this is true?But Nivek, if you test everyone, you're only going to find that almost everybody has it ...except, as you mention, a very small number of truly immune.
I think a significant minority of the population in several countries has it. Taking the estimated mortality rates of the Stanford study Thomas mentioned a few posts up (0.12-0.2%), it could be the case that 8-14 million Britons were infected cumulatively by the virus 4 weeks ago. I don't know how many have been infected since then, presumably not as many because the country has been fairly vigorously obeying the lockdown (apart from the odd example of stupid behaviour). Using the fatality rate estimates of 0.66-1% (I am detecting an institutional bias at Stanford to give lower estimates of the mortality rate), then that would be 1.6-2.4 million cumulative infections four weeks ago.
And of those cumulative infections, many will be over the infection by now, so will only have had it, not have it. At the upper range of 14 million, that is only about 22% of the total population of Britain. So the majority have likely yet to be exposed to the virus.
nivek
As Above So Below
I'm very encouraged to see that small-scale study reporting successful outcomes with convalescent plasma: it sounds like they were able to pull several of those ten people back from the brink with just one injection. That's exactly what we need: a treatment that we can give to the most severe cases, and ideally reduce the chances of death in severe cases down to a few percent or less. Because that's what's really scaring the shit out of everyone: knowing that if this virus hits you hard and you get ARDS, then there's nothing they can do but put you on a ventilator and you'll have about a 20% chance of surviving.
It is not much to ride on but does offer a slight bit of hope...I hate to sound dark in this other thread but I do prefer to face problems directly and see it as it is and currently we do not have much on our side to stop this virus...Sure there are many labs across the world working on this problem but time is of the essence too...
But Nivek, if you test everyone, you're only going to find that almost everybody has it ...except, as you mention, a very small number of truly immune.
I think the percentage may go up to 15 or 20 percent at the most if we were to test everyone across the world promptly but I doubt almost everyone has it or had it at one point...The question also arises that if we do have people who are immune, are they immune to one strain or mutation or all of them?...The more people exposed increases the likelihood of more mutations, those immune now may not be immune a months or six months from now...Are there also varying degrees of illness from this virus?...Could an individual get a mild illness from this virus and get well but get it again much harder the second time, perhaps hospitalizing him or her?...
There is this study here from 1990:
The time course of the immune response to experimental coronavirus infection of man.
The researchers inoculated 15 volunteers with coronavirus 229E, ten became infected, eight developed colds. 14 of these were able to return a year later to be re-inoculated. The group of five originally uninfected became infected this time, and one developed a cold. Of 9 returning volunteers in the infected group, six became infected on inoculation and shed virus, but did not develop disease (i.e. they were potentially asymptomatic spreaders).
I think that the degree and duration of immunity conferred by antibodies will vary across the population because not everyone has the same immune response. Some diseases have a much better immune response that is more uniform across the population than others.
For the results in regards to SARS-Cov-2, there was this report on a medical pre-print from China that I posted a couple of weeks ago:
Low antibody levels raise questions about coronavirus reinfection risk
The pre-print is here:
Neutralizing antibody responses to SARS-CoV-2 in a COVID-19 recovered patient cohort and their implications
Researchers measured SARS-Cov-2-specific neutralizing antibody levels in recovered mild Covid-19 cases. They found that a third had levels that might be insufficient to prevent re-infection, and in some patients they could not detect antibodies. The researchers excluded severe cases because they could have been in receipt of antibody-containing blood plasma. The older patients tended to have a greater presence of neutralizing antibodies than younger ones.
The idea that those vulnerable to the severe illness will be able to rely upon the herd immunity offered by those less vulnerable therefore seems questionable to me. It also makes a vaccine's likelihood of succeeding similarly questionable. Some vaccines are able to prevent disease in an individual, but not infection, allowing them to keep spreading it. This was the cause of an argument between the WHO and China about 15 years ago, because the Chinese were vaccinating chickens against avian influenza, but their vaccines were only able to prevent disease in chickens, and not infection. This enabled asymptomatic spread and provided a breeding ground for avian flu to mutate into more dangerous strains.
We can only hope that there are other immune mechanisms at work that provide immunity to SARS-Cov-2 and that a vaccine will be successful, but assuming things is dangerous.
I am correct to surmise that those who get well from receiving plasma treatment have the possibility of getting Covid-19 again?...
...
nivek
As Above So Below
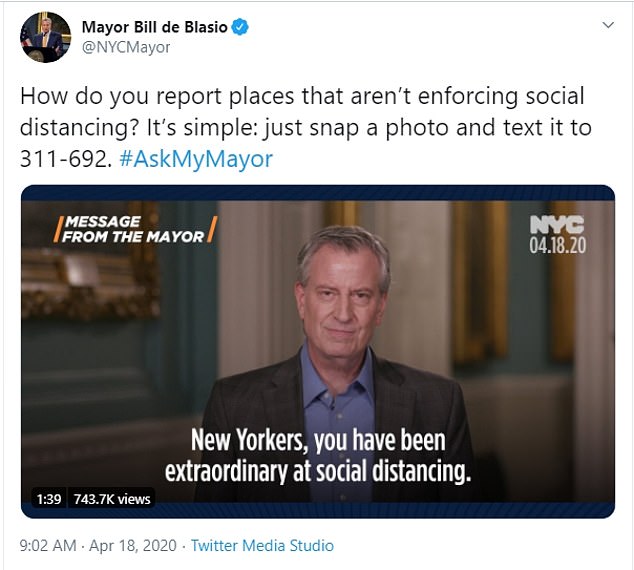
'This is so un-American': Mayor Bill de Blasio is slammed on social media after he urges New Yorkers to SNITCH on those not social distancing by snapping their photo and texting it to the city
Mayor Bill de Blasio wants New Yorkers to rat out their fellow citizens who are not following social distancing orders during the coronavirus pandemic by taking a photo of the violators on their cell phones and texting it to the city.
'It's simple: just snap a photo and text it to 311-692,' the mayor tweeted Saturday. In a video posted to his Twitter account, de Blasio praised the people of his city, saying: 'You have been extraordinary at social distancing.'
Mayor Bill de Blasio wants New Yorkers to rat out their fellow citizens who are not following social distancing orders during the coronavirus pandemic by taking a photo of the violators on their cell phones and texting it to the city.
'It's simple: just snap a photo and text it to 311-692,' the mayor tweeted Saturday. In a video posted to his Twitter account, de Blasio praised the people of his city, saying: 'You have been extraordinary at social distancing.'

nivek
As Above So Below
Are we overreacting to the coronavirus? Let’s do the math
Is the economic cost of COVID-19 $150 billion? Or $5.6 trillion?
As coronavirus deaths and infections plateau in many parts of the country, and as the economic damage of stay-at-home orders mounts, a question is gaining ground: Are we overreacting?
Some economists and business leaders believe the costs of constraining the virus have exceeded the benefits. They point to unemployment totals not seen since the Depression and entire industries shut down, compared to virus death totals that may reach only the numbers from a bad flu season (55,000).
As more data become available, the epidemiological trajectory of the virus is becoming clearer, allowing us to estimate the costs of COVID-19 and whether government restrictions are worth the price we are paying.
Serology results suggest that about 3% of the U.S. population is infected, 1 in 10 of whom will be hospitalized (based on New York City data), and 1 in 200 of the infected dying (0.5% mortality rate or about 5 times the flu). Economists can use those numbers as part of a cold-eyed calculation that includes the economic value of a life year.
By looking at what we are willing to pay to reduce the risk of death—for example, how much will we pay for a smoke detector at home or air bags in the car—economists assign a dollar figure to a life year, now typically measured at $150,000. Applying that measure to the age distribution of the deceased, and adding the costs of treating the infected population, the total cost of COVID-19 in the U.S. under current restrictions appears to be about $150 billion. This estimate pales in comparison to the $2.3 trillion stimulus package alone and seems to support Wisconsin Sen. Ron Johnson’s recent concern that “the cure is worse than the disease”.
But what would the cost be if governments had not imposed restrictions and simply let the virus run its course? Suppose, if unchecked, 30% of Americans became infected, far below most estimates, including California Gov. Gavin Newsom’s projection that 56% of his state’s residents would be infected without mitigation. Applying the same rates of hospitalizations and mortality to this higher rate of prevalence increases the cost of COVID-19 to nearly $3 trillion. And if we assume, quite reasonably, that mortality rates would rise from 0.5% to 1.5% as hospitals become increasingly overrun, the estimated cost of COVID-19 increases to $5.6 trillion, by my calculations.
Just like a pandemic, the economic toll is not linear. Small additional increases in prevalence and mortality rates lead to spiraling cost estimates that quickly reach tens of trillions of dollars.
Given the country’s delayed response to the virus that allowed it to spread unchecked in February and into March, the government had no choice but to restrict social interaction and close down nonessential activity. The costs of not doing so would very likely have been far greater than the economic toll we’re experiencing. Certainly the risk of a catastrophe was mounting by the day.
Coronavirus-related restrictions have worked, as the number of new cases and deaths begin to recede and the debate shifts toward finding an appropriate balance between continued mitigation and restarting the economy. Americans’ ambivalence over how to proceed was on full display over the past week, as impatience with prolonged stay-at-home orders led to protests in several capitals, while the newly formed task force led by banking and financial services executives told President Trump that the public would not return to work, eat at restaurants and shop like before unless testing for the virus was dramatically increased
When the virus threat is over, the second-guessing on every policy step and misstep will be cacophonous. But we should remember that when the risk is extreme, such as it is for global warming or COVID-19, public policies should be based on credible worst-case scenarios. Too much is at stake to act otherwise.
.
Is the economic cost of COVID-19 $150 billion? Or $5.6 trillion?
As coronavirus deaths and infections plateau in many parts of the country, and as the economic damage of stay-at-home orders mounts, a question is gaining ground: Are we overreacting?
Some economists and business leaders believe the costs of constraining the virus have exceeded the benefits. They point to unemployment totals not seen since the Depression and entire industries shut down, compared to virus death totals that may reach only the numbers from a bad flu season (55,000).
As more data become available, the epidemiological trajectory of the virus is becoming clearer, allowing us to estimate the costs of COVID-19 and whether government restrictions are worth the price we are paying.
Serology results suggest that about 3% of the U.S. population is infected, 1 in 10 of whom will be hospitalized (based on New York City data), and 1 in 200 of the infected dying (0.5% mortality rate or about 5 times the flu). Economists can use those numbers as part of a cold-eyed calculation that includes the economic value of a life year.
By looking at what we are willing to pay to reduce the risk of death—for example, how much will we pay for a smoke detector at home or air bags in the car—economists assign a dollar figure to a life year, now typically measured at $150,000. Applying that measure to the age distribution of the deceased, and adding the costs of treating the infected population, the total cost of COVID-19 in the U.S. under current restrictions appears to be about $150 billion. This estimate pales in comparison to the $2.3 trillion stimulus package alone and seems to support Wisconsin Sen. Ron Johnson’s recent concern that “the cure is worse than the disease”.
But what would the cost be if governments had not imposed restrictions and simply let the virus run its course? Suppose, if unchecked, 30% of Americans became infected, far below most estimates, including California Gov. Gavin Newsom’s projection that 56% of his state’s residents would be infected without mitigation. Applying the same rates of hospitalizations and mortality to this higher rate of prevalence increases the cost of COVID-19 to nearly $3 trillion. And if we assume, quite reasonably, that mortality rates would rise from 0.5% to 1.5% as hospitals become increasingly overrun, the estimated cost of COVID-19 increases to $5.6 trillion, by my calculations.
Just like a pandemic, the economic toll is not linear. Small additional increases in prevalence and mortality rates lead to spiraling cost estimates that quickly reach tens of trillions of dollars.
Given the country’s delayed response to the virus that allowed it to spread unchecked in February and into March, the government had no choice but to restrict social interaction and close down nonessential activity. The costs of not doing so would very likely have been far greater than the economic toll we’re experiencing. Certainly the risk of a catastrophe was mounting by the day.
Coronavirus-related restrictions have worked, as the number of new cases and deaths begin to recede and the debate shifts toward finding an appropriate balance between continued mitigation and restarting the economy. Americans’ ambivalence over how to proceed was on full display over the past week, as impatience with prolonged stay-at-home orders led to protests in several capitals, while the newly formed task force led by banking and financial services executives told President Trump that the public would not return to work, eat at restaurants and shop like before unless testing for the virus was dramatically increased
When the virus threat is over, the second-guessing on every policy step and misstep will be cacophonous. But we should remember that when the risk is extreme, such as it is for global warming or COVID-19, public policies should be based on credible worst-case scenarios. Too much is at stake to act otherwise.
.